
Document Type : Case Report
Introduction
Cavernous hemangiomas are benign vascular adrenal masses that are very rare and comprise approximately 0.01% of adrenal masses. Their presentation is usually an accidental finding in imaging. Its most common clinical symptom is non-specific and vague abdominal pain. Differentiating from malignant adrenal masses remains challenging, and the diagnosis is usually made after surgery. Here, we report an adrenal hemangioma in a 60-year-old woman, which was found incidentally during lung computed tomography (CT) scan.
Case Presentation
A 60-year-old female patient presented with dyspnea,which was subsequently attributed to bronchiectasis. During a routine lung computed tomography (CT) scan, incidental imaging of the upper abdomen revealed a left adrenal mass measuring 40 mm in diameter with a Hounsfield Unit (HU) value exceeding 10. The patient reported no associated symptoms such as flank pain, hypertension, or headaches.
Further diagnostic imaging was performed, including an adrenal wash out CT protocol. The latter confirmed a well-defined mass originating from the left adrenal gland, measuring 35x40 mm. The lesion exhibited calcified components and heterogeneous enhancement, with a relative washout of <40% and an absolute washout of <60%. These imaging characteristics were inconsistent with a benign adrenal adenoma.
To exclude functional adrenal pathologies, a comprehensive panel of adrenal function tests was conducted. The results, summarized in Table 1, were all within normal ranges, effectively ruling out pheochromocytoma.
Table 1. Adrenal Function Tests Result
|
Test Parameter |
Value |
Normal Range |
|
24h Urine Metanephrine |
174 μg/day |
140-785 μg/day |
|
24h Urine Normetanephrine |
567 μg/day |
<600 μg/day |
|
24h Urine VMA |
2 mg/24h |
<7 mg/24h |
|
24h Urine Free Cortisol |
16.2 μg/day |
<45 μg/day (female) |
|
Aldosterone |
13.9 ng/dL |
3-25 ng/dL |
|
Plasma Renin Activity |
0.16 ng/mL/hr |
0.7-3.3 ng/mL/hr |
Given the suspicion of adrenal malignancy, an open left adrenalectomy was performed under general anesthesia with the patient positioned in left lateral decubitus. The procedure was initiated via a left flank incision using a retroperitoneal approach. Initially, the patient's hemodynamics were stable with a blood pressure of 135/85 mmHg. However, during adrenal gland manipulation, an acute hypertensive crisis occurred with the blood pressure spiking to 210/110 mmHg and heart rate increasing from 72 to 115 bpm.
Immediate adrenal vein ligation was performed; however, this intervention did not result in significant blood pressure reduction. Consequently, the anesthesiologist initiated an intravenous nitroglycerin (TNG) infusion. Following adrenal gland removal and cessation of TNG, the patient's systolic blood pressure surged to 220/120 mmHg. TNG infusion was reinstated and titrated to maintain systolic pressure between 120-140 mmHg.
Post-operatively, the patient was transferred to the intensive care unit (ICU) for close hemodynamic monitoring. In the initial 24 postoperative hours, multiple attempts to wean TNG were unsuccessful, with dose reductions consistently resulting in hypertensive responses. From the second postoperative day, gradual TNG tapering was achieved, and the infusion was eventually discontinued on day 3.
The patient's blood pressure subsequently stabilized within normal limits (130-140/80-90 mmHg) without pharmacological intervention. On day 3, the patient was transferred to the general ward and was discharged home on day 7 with normal blood pressure and no antihypertensive medications.
Follow-up at six months post-surgery demonstrated sustained normotension with an average blood pressure of 125/75 mmHg. The patient's pulmonary symptoms had also improved with ongoing management of her bronchiectasis.
Histopathological examination of the adrenal lesion, reported approximately two weeks postoperatively, revealed a well-circumscribed, dark red-brown mass measuring 3.8 x 3.5 x 3.2 cm. Microscopic analysis showed large, dilated vascular channels lined by flat endothelial cells. Immunohistochemistry was positive for CD31 and CD34 in endothelial cells. The final diagnosis was adrenal cavernous hemangioma.
The patient was a 60-year-old woman who underwent lung CT scan due to Dyspnoea which later was found to be due to bronchiectasis. . In limited cuts from the upper part of the abdomen, a 40 mm left adrenal mass with HU>10 was seen in the lung CT scan. The patient did not mention any related complaints such as flank pain, increased blood pressure, headache, etc. The patient underwent further investigation (Figure 1-4).
Fig1. Spiral lung CT Scan Without contrast
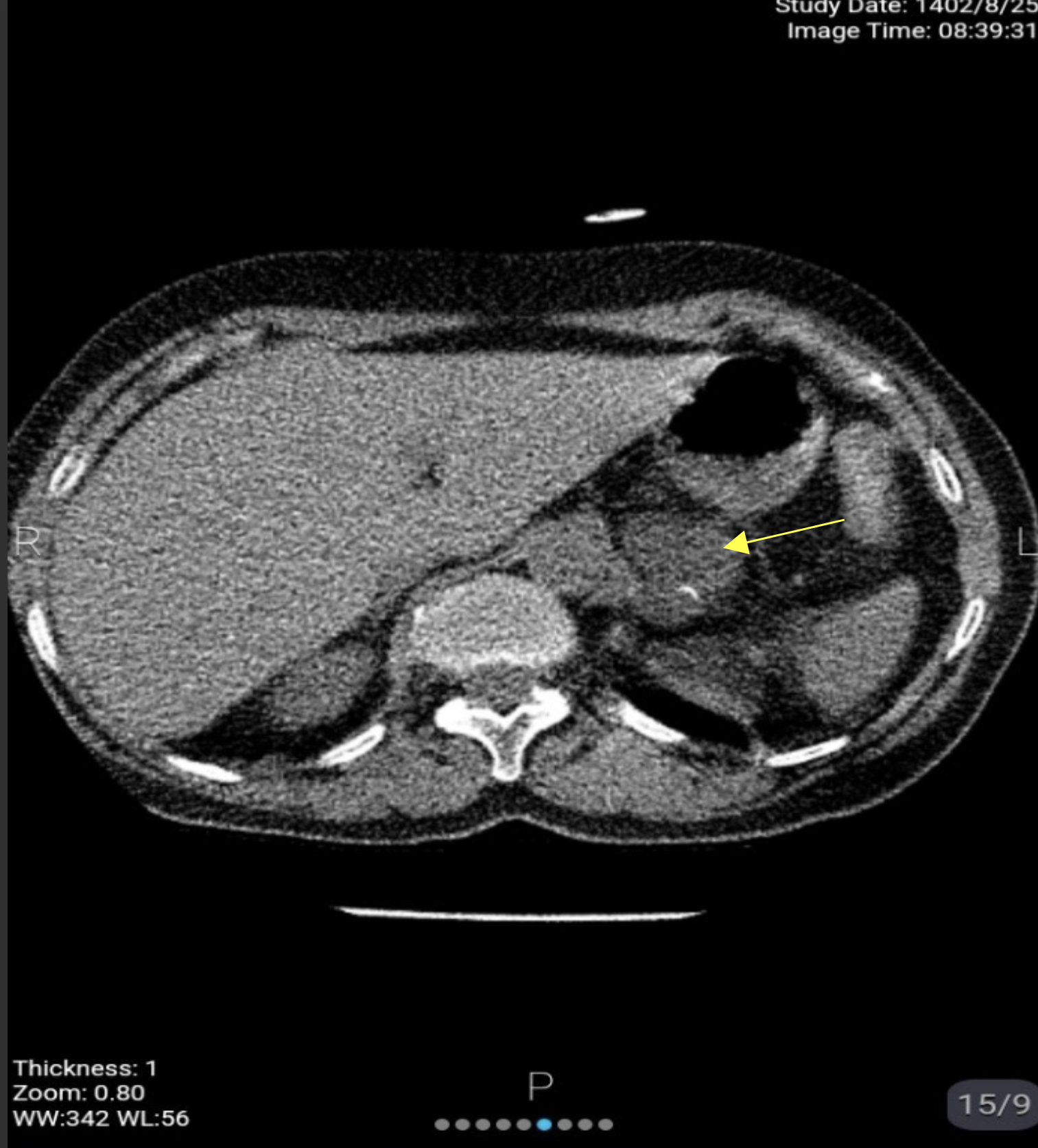
Fig2. Spiral abdominopelvic CT Scan without and with intravenous contrast
.%5B4%5D.png)
Fig3. Spiral abdominopelvic CT Scan without contrast
.%5B1%5D.png)
Fig4. Spiral abdominopelvic CT Scan with intravenous contrast
.%5B1%5D.png)
Suspecting an adrenal malignancy, the patient underwent open left adrenalectomy surgery. The patient’s position was left lateral decubitus. At the beginning of the surgery, the patient's blood pressure was under control in the normal range below 140/90 mmhg.
The surgery started with a left flank incision. Blood pressure was within normal range during surgery. After finding the adrenal gland while manipulating it in order to dissect it from the surrounding attachments, the patient had a blood pressure crisis. We immediately ligated the adrenal vein with double tie. No significant change was seen in blood pressure so the anaesthesiologist started TNG drip for the patient, leading the SBP to reach 60 mmhg. In the meantime, the adrenal gland was removed (Figure 5), and after stopping TNG, the patient's pressure reached 220 mmhg . With the help of TNG, the patient's systolic blood pressure was maintained in the range of 120-140 mmhg, and after the surgery, the patient was transferred to the ICU with a TNG drip in good general condition. During the first 24 hours after the operation, the attempt to taper TNG was not successful, and every time the reduction of the TNG dose was accompanied by an increase in the patient's blood pressure, eventually from the second day, the TNG drip was tapered and finally stopped, and the patient's blood pressure was maintained within the normal range without medica-tion. Then the patient was transferred to the inpatient ward. She was discharged after 5 days without any complications.
Fig5. Resected en-block of tumor
.png)
After the surgery, the patient was followed up until 6 months later, and the blood pressure remained within the normal range. The pathology result was reported about 2 weeks later and the patient’s adrenal lesion was identified as covernous hemangioma. (Figure 6-7).
Fig6. Left adrenal gland with a hemorrhagic solid lesion corresponding to adrenal hemangioma
.%5B1%5D.png)

Fig7. Cross section of the mass: microscopic image showing haemangioma


Section show adrenal tissue composed of intact Cortex and Medula which is involved by a neoplasm composed of dilated congested and thrombotic combined thin walled and hyalinized vessels lined by flatted endothelial cells. Stromal hyalinizatin, calcification and RBC extravasation are also noted. Adrenal mass Consistent with cavernous hemangioma
Discussion
Hemangiomas are benign vascular masses ariginated from the endothelial layer of vessels, which are usually seen in the skin and liver (1). Pathologically, hemangiomas are divided into two subgroups, cavernous and capillary, and the cavernous type is more common and is seen as a large mass with sinusoids covered with endothelium and containing blood (2). Adrenal cavernous hemangiomas are benign and rare lesions that constitute about 0.01% of adrenal masses.¹ Since 1955 when this mass was first reported by Johnson and Jeppsen,(3). until the time of writing this report, less than 140 cases of it have been reported in articles. Among the known cases, there is a slight male predominance, and the average age of the patients at the time of diagnosis was 60 years. Masses are often unilateral and patients are often asymptomatic or have vague non-specific abdominal pain. The mass is mainly discovered as Incidentaloma (4). Cavernous hemangiomas have no endocrine activity (5). This issue was consistent with our patient's adrenal functional tests, which were all within normal limits. In this patient, contrary to expectations, during the surgery, the systolic blood pressure reached about 200 mmhg after manipulating the adrenal gland, which was suspicious for the diagnosis of pheocrocytoma. However, the lack of reduction in blood pressure after ligating the adrenal veins was not consistent with this diagnosis. Ultrasound and CT scan findings are non-specific for the diagnosis of adrenal cavernous hemangioma. However, in Peng et al.'s study on 10 cases of adrenal hemangioma, it was seen that in the presence of a well marginated heterogeneous adrenal mass with calcification and various enhancement patterns, adrenal hemangioma should be iconsidered as a differential diagnosis. Enhancement patterns can include heterogeneous enhancement with incomplete internal filling or lack of enhancement in any of the phases (6). Calcification in the mass can favor the diagnosis of hemangioma, although this finding is also seen in neoplasms and cysts (7). The calcification pattern can be speckled in a large mass or in the form of radial branches from the center of the mass. Also, a crescent-shaped calcification pattern may be seen. In MRI images, adrenal hemangiomas are similar to liver and spleen hemangiomas and are seen as hypointense in T1w and hyperintense in T2w (8). Focal hyperintense areas in T1w may also be seen as a result of bleeding or calcification (1).
Conclusion
Cavernous hemangioma of adrenal is a very rare benign vascular adrenal mass. mostly diagnosed after removal surgery and pathology result. Its radiological feature is described as well defined heterogeneous adrenal masses with calcification and mainly peripheral small rim of enhancement. regarding that, it might be possible to diagnose the disease before the surgery by radiological manifestation. In this case cavernous hemangioma of adrenal caused unstable blood pressure during the surgery in a patient with no past history of hypertension, suggesting that even if the adrenal functional tests were negative, its always a wise decision to be prepared for wide blood pressure fluctuation.
Acknowledgments
The authors thank and appreciate the cooperation of Sekineh kamali Ahangar the expert of Clinical Research Development Unit of Shahid Beheshti Hospital of Babol.
References
1. Zemni I, Haddad S, Hlali A, Manai MH, Essoussi M. Adrenal gland hemangioma: A rare case of the incidentaloma: Case report. Int J Surg Case Rep. 2017 Nov 16; 41:417-422. doi: 10.1016/j.ijscr.2017.11.021. PMID: 29546006; PMCID: PMC5702858.
2. Hamrick - Turner J. E., Grider P.L., Allen B.C.,
Fowler J.E., Cranston P.E., Harrison R.B. Adrenal hemangioma: MR findings with pathologic correlation. J Comput Assist Tomogr. 1993; 17(3):503–505.
3. Johnson CC, Jeppesen FB. Hemangioma of the adrenal. J Urol. 1955; 74:573–577.
4. Toklu A, Mesa H, Collins K. Incidental adrenal hemangioma clinically suspicious for malignancy: diagnostic considerations and review of the literature. Int J Clin Exp Pathol. 2022 Nov 15; 15(11):444-458. PMID: 36507066; PMCID: PMC9729942.
5. Al-Rawashdah S, Mansi H, Pastore AL, Carbone A. Adrenal cavernous Hemangioma;A rare diagnosis of adrenal incidentaloma:A case report, and literature review. Urol Case Rep. 2020 Oct 31; 34: 101477. doi: 10.1016/j.eucr.2020.101477. PMID: 33204642; PMCID: PMC7653277.
6. Peng JP, Lv XF, Lin CL, et al. Computer tomography imaging findings of adrenal cavernous hemangiomas: A report of 10 cases. Acta Radiol. 2016; 57(1):115–21.
7. Almajed EH, Alshamrani AM, Alqahtani AS, Alzahrani AJ, Alahmadi T, Asiri SM. Rare Case of Adrenal Hemangioma Discovered Incidentally during Renal Colic Investigation. Am J Case Rep. 2024 Jul 5; 25: e943826. doi: 10.12659/AJCR.943826. PMID: 38965761; PMCID: PMC11322789.
8. Edwards JP, Stuart HC, Urbanski SJ, Pasieka JL. A rare cavernous hemangioma of the adrenal gland. Int J Surg Case Rep. 2014; 5(2):52-5. doi: 10.1016/j. ijscr. 2013. 11.003. Epub 2013 Nov 20. PMID: 24441435; PMCID: PMC3921650.
